How Doppler Detects Blood Flow
Blood flow in veins is pulsatile and driven by heart cycle dynamics. Regardless of cardiac abnormality, it is still possible to accurately place lines in the lower 1/3 of the SVC-CAJ by assessing blood flow.
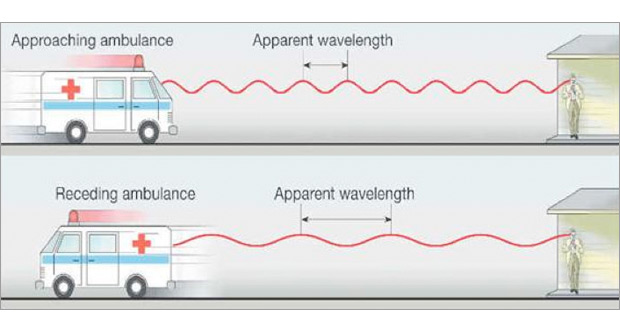
The Doppler Effect is well known to anyone who has listened to a passing vehicle. Although the sound waves are emitted at the same frequency at their source, the received frequency is higher (compared to the emitted frequency) during the approach. It is identical at the instant of passing by, and it is lower during the recession. The reason for this is that the sound waves emitted in the direction of the moving vehicle are compressed whereas those emitted in the opposite direction are "spread out."
The ARROW® VPS G4™ Device uses a Doppler microsensor that emits sound waves as the catheter is moved through the vein. These sound waves are reflected back by the red blood cells (RBCs), giving information on the direction and velocity of the blood flow. If the RBCs are going in the same direction as the catheter, the wave frequency reflected back to the microsensor will be longer than if they are moving toward the microsensor.
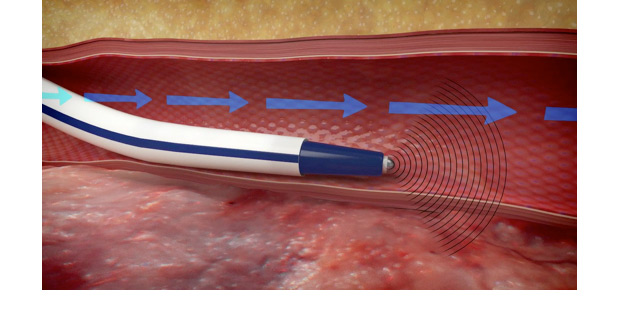
The ARROW VPS G4 Device can detect antegrade blood flow as the catheter navigates through the vein towards the lower 1/3 of the SVC-CAJ, and retrograde flow if the catheter is moving into one of the feeder veins away from the target (e.g., internal or external jugular, contralateral, azygos). In this manner, the clinician uses the combination of the ARROW® VPS G4™ Device symbols and the Doppler and ECG waveforms for navigational guidance and precise tip placement.

Characteristics of ECG and Doppler waveforms according to the anatomical position of the ARROW ®VPS® Stylet in the central venous system
| Anatomical Location | ECG | Doppler |
|---|---|---|
| Upper Vasculature | Regular ECG or distorted waveform due to Stylet movement | Doppler waveform small (lower amplitude, less steep) |
| Confluence of Two Veins | No specific changes | May see transient turbulence, below baseline (audible and visible). May see intermittent Orange Symbol, e.g. Internal Jugular vein |
| Proximal/Mid SVC | Regular ECG P-Wave might grow slightly R-Wave often grows |
Pulse waves taller and steeper with two antegrade peaks (Systolic/Diastolic) and distinct small retrograde wave. |
| Distal SVC-CAJ | P-Wave grows visibly All other ECG waves can increase |
Several types of bloodflow signatures, with increased turbulent activity around the baseline. Most common pulsatile, "cathedral" type waveform. |
| CAJ | May not see significant change of P-Wave as catheter tip moves from lower 1/3 SVC to CAJ (see Distal SVC-CAJ). |
Increasing retrograde Doppler signature. RA turbulent elements. Waveforms are distinct in upper CAJ. |
| RA | P-Wave inconsistent, could be maximal, decreasing or Bi-phasic. Higher amplitude in other parts of ECG. | Intense turbulence, usually retrograde dominant or combination. Loss of pulsatile sound, similar to sound of white noise. |